
COTW 9/17/2022: A 54 year old male history of metastatic colon cancer presenting with shortness of breath
A 54 year old male history of metastatic colon cancer presents for evaluation of shortness of breath x 3 days. He denies fevers, chest pain, sputum production, orthopnea or leg swelling.
His vitals are:
BP 121/89 HR: 102 RR: 19 SpO2: 99% T 99.2 F
Examination shows a relatively comfortable man with some very mildly increased work of breathing. No pedal edema is appreciated.
The differential for this patient is very, very broad. Thankfully you are wise and decide to echo your patient to gather some more information.
Moderate sized pericardial effusion with RV diastolic collapse
Apical 4 also showing right ventricular diastolic collapse
IVC with minimal respirophasic Variation
What features of these images suggest tamponade?
IVC dilation is the most sensitive finding(around 95%) and has a high negative predictive value. However it is poorly specific as many pathologies can cause IVC dilation.
Diastolic collapse of the RV is more specific to tamponade but less sensitive than IVC dilation. This occurs because early in diastole, the Right sided intraventricular pressure is less than the pressure exerted by the surrounding pericardial effusion which then leads to collapse.
People will often describe this as if someone is jumping on the trampoline of the RV free wall during diastole and causing it to collapse as illustrated(to the best of my abilities) below

While not terribly difficult to see the RV diastolic collapse in the initial clips, it becomes harder to appreciate the more tachycardic your patient is. M-Mode is a great tool to use whenever you are unsure. It can also help you potentially catch more subtle cases of tamponade.
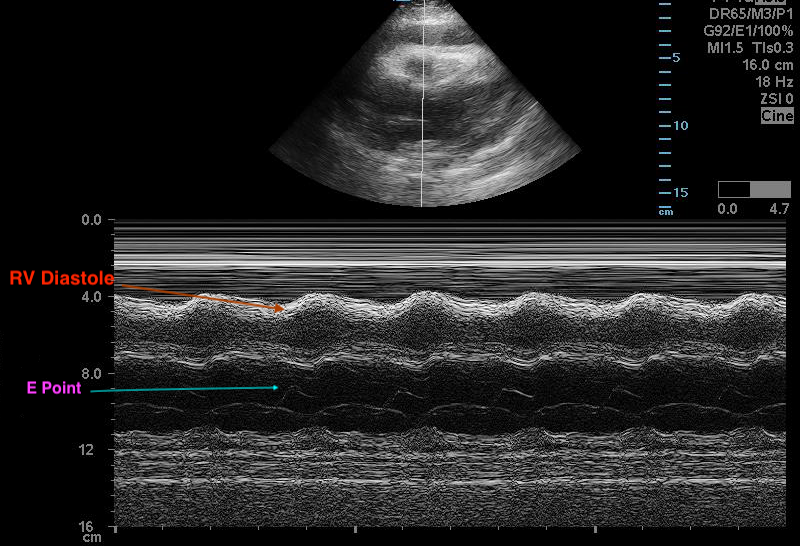
To do this, you are going to place your M Mode cursor over the mitral valve leaflet like you are going to calculate EPSS. Identify the E point, which is the point that the mitral valve is closest to the intraventricular septum. Draw an imaginary vertical line from the E point to the tracing of the RV Free wall. This is seen oscillating around 4 cm in depth throughout the cardiac cycle and its location during diastole is labeled above. You can see that as the mitral valve opens during diastole, the RV free wall appears to be collapsing, suggesting tamponade.
BACK TO THE CASE:
Based on your quick bedside ultrasound, you arrange for your patient to be transferred to a facility with interventional cardiology. Shortly after arrival at the outside hospital he develops some work of breathing and mild hypotension that improves with a small IV fluid bolus. He is taken to the interventional cardiology suite and has a pericardial drain placed and discharged a few days later. As you read up on the case outcome you thank the POCUS gods for their powers. Your patient would have likely had a much different outcome if you had not started your workup with an echo.