
COTW 12/27/22: 54F with R hand pain, swelling, erythema
54yo F presents to the ED with right hand pain, redness and swelling progressive over the last two days. Patient sustained multiple small dog bite puncture wounds when she was trying to break up a fight between her two dogs. Puncture wounds were located on the both palmar and dorsal aspect of the radial side of the patient’s hand, with the pain and swelling mostly around the thenar eminence. Patient was also having difficulty moving her thumb and wrist. Patient was afebrile with normal vitals. On exam, she had significant tenderness to palpation with redness and swelling worse over the thenar aspect of her hand with extension throughout the thumb.
This case is not a medical mystery but is a great example of how using ultrasound can help you pinpoint your diagnosis. In this case, we are trying to differentiate between cellulitis vs abscess vs flexor tenosynovitis vs septic joint. Using a water bath is extremely helpful to facilitate scanning the distal extremities.

Why use a water bath?
As we know, fluid is highly effective in transmitting sound waves. Using a water bath can help you get a better image without the probe needing to be in full contact with the patient’s skin. This helps reduce the pain associated with the exam, as well as minimizes distortion of superficial tissues from the pressure of the probe on the skin.
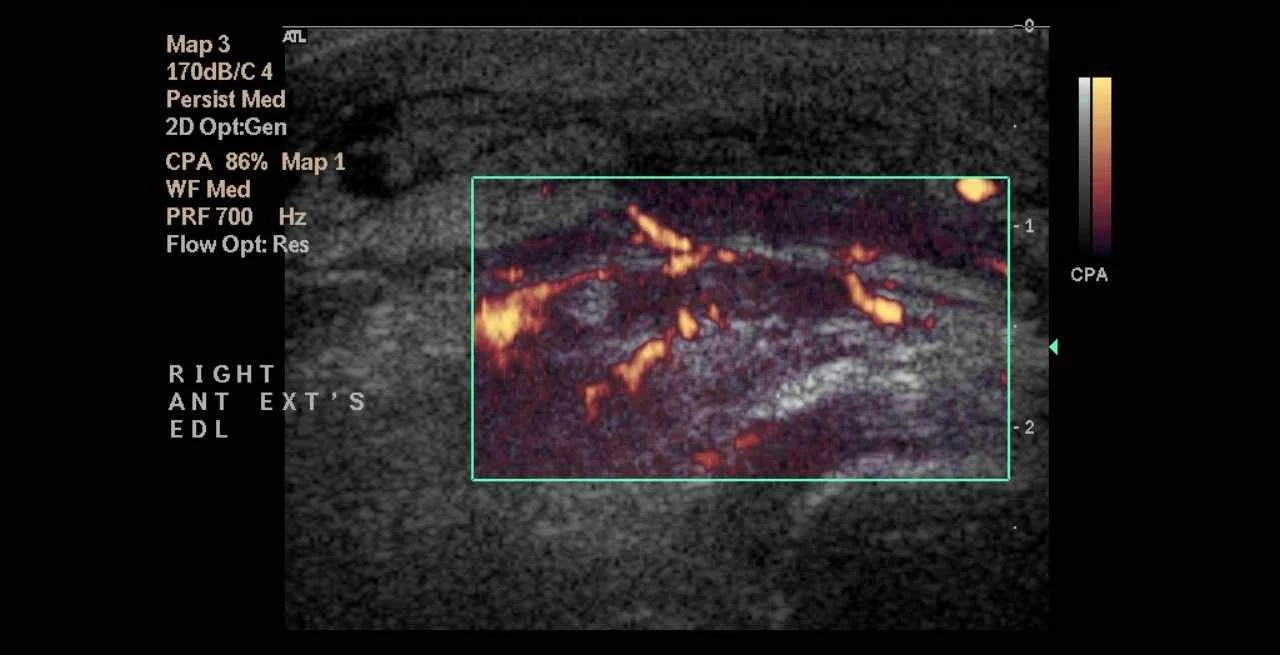
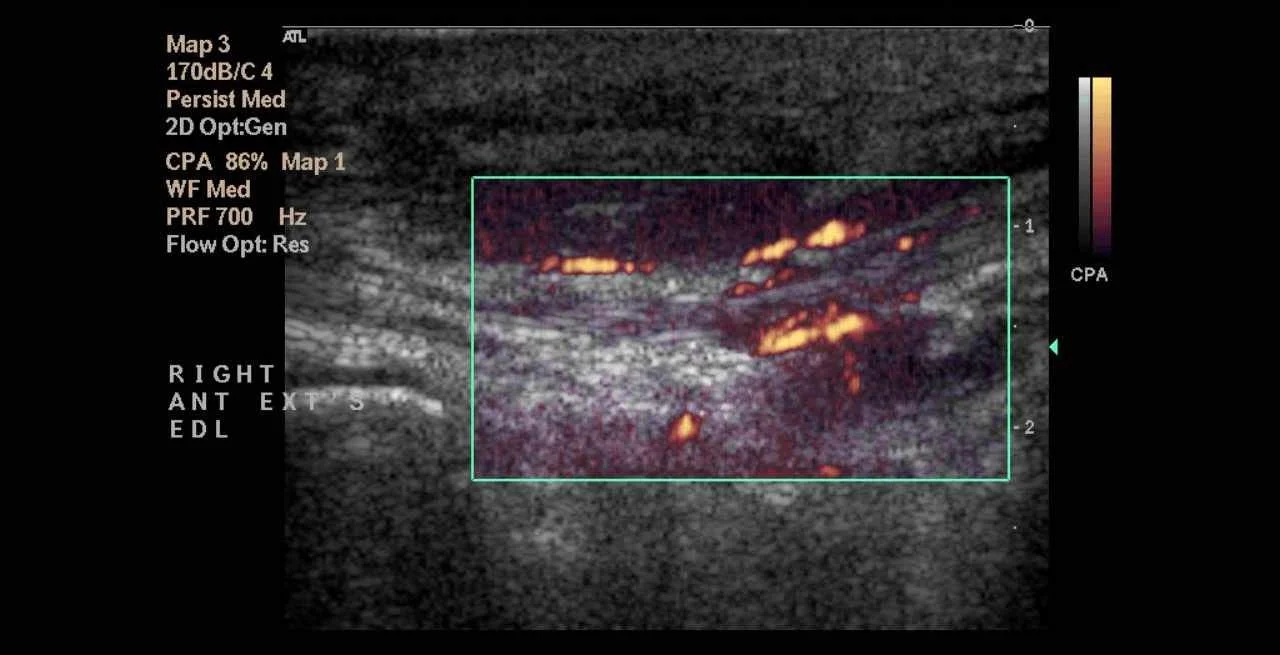
Scanning the patient’s thenar eminence in both long and short access gives you the images below.


It is easy to appreciate an anechoic / hypoechoic rim layering above and below a fibrillar structure (top, longitudinal view) and encircling a circular / ovoid structure (bottom, transverse view) with a hyperechoic cluster of dots, seen best at the end of the clip. These structures are the flexor tendon. Tendons are high anisotropic so these characteristic patterns will be seen best when the ultrasound beam is perfectly perpendicular to the tendon. Other signs that may be present on ultrasound are a thickened hypoechoic synovial sheath and a hyperemic rim around the tendon when viewed with color doppler.

Images above courtesy of Yaïr Glick, Radiopaedia.org, rID: 73683
Of note, effusions (particularly small ones) can be easily compressed, and therefore missed, thus highlighting why it is important to apply as little pressure as possible (ie use a water bath) when doing your evaluation.
The photo below (not the same patient as described in our case) shows what you would expect to see clinically.


When thinking about flexor tenosynovitis, don’t forget the four Kanavel sign’s listed above. Studies show that the presence Kanavel’s signs has a sensitivity of 91-97% for FTS - but only if you have all 4. One large study of 57 cases of FTS conducted by Jardin et al in 2018 (doi:10.1016) showed the ultrasound has 94% sensitivity, 65% specificity, 63% positive predictive value, and 95% negative predictive value in diagnosing FTS.
The earliest sign is often pain on passive extension so you may not see extensive outward swelling in early presentations (another plug for why ultrasound can be extremely useful aiding in this diagnosis). Don’t forget, fever is usually absent.
In our case, orthopedics was consulted given the ultrasound findings, and the patient was given IV antibiotics x1, then transitioned augmentin and scheduled to return for follow up in ortho clinic in 1-2 days.